
Sepsis is a lethal disease caused by a systemic microbial infection. This disease is a major killer of premature infants, immuno-compromised patients and citizens of many undeveloped nations. The overall death rate from this blood infection is over 25% in the US, and it is even higher internationally. The treatment of patients with sepsis also incurs a heavy economic burden: costs can be as high as $50,000 per patient and approximately $17bn is spent annually in the US to treat and manage patients with this disease.
The lethality of sepsis is triggered by an overload of the immune system due to rapidly growing pathogens that utilise the bloodstream to spread throughout the body. A ‘tipping-point’ is reached when the body’s natural clearance mechanisms are overcome. This ignites widespread inflammatory responses and therapies are then no longer effective, as clot formation, hypoperfusion, shock, multiple organ failure and death ensue.
Go deeper with GlobalData

Discover B2B Marketing That Performs
Combine business intelligence and editorial excellence to reach engaged professionals across 36 leading media platforms.
Treating sepsis
Patients with sepsis and septic shock are commonly treated with antibiotics, intravenous fluids, vasopressors, and, if necessary, packed red blood cells to restore blood pressure and oxygen saturation. Other therapies include anti-inflammatory and anti-thrombotic drugs or hemofiltration and hemadsorption treatments to remove inflammatory mediators (tumour necrosis factor, interleukin-1) with the goal of suppressing the damaging inflammatory cascade.
However, these methods do little to rid the patient of the living pathogens that are the primary source of toxins and continually activate this devastating inflammatory cascade. Excessive removal of pro-inflammatory mediators also can have a negative impact on patient outcome because many of these same mediators are required to combat the pathogens that still multiply within the body.
Because of the dominant focus on the systemic inflammatory response, most clinicians and investigators have essentially ignored the possibility that removal of pathogens from the blood could reverse the septic process. However, some patients with fulminant septicemia respond well to antibiotic therapy alone, which acts exclusively by reducing the pathogen load. Moreover, there have been anecdotal clinical cases in which septic neonates with documented infections of the blood have been saved by removing the patients’ entire blood volume and replacing it with an equal volume of packed red blood cells.
Unfortunately, generalised use of whole blood transfusion is limited because removal of endogenous white cells, platelets, antibodies and other blood components leads to complications, including decreased immunoreactivity and an increased risk of infection (HIV, Hepatitis C). These observations suggest that a device that can rapidly cleanse the blood of pathogens without removing critical normal blood cells, proteins, fluids or electrolytes could save the lives of many septic patients.
Pathogen removal
Don Ingber, a professor at the Boston Children’s Hospital, Harvard Medical School and Harvard School of Engineering and Applied Sciences, is the principal investigator of a translational research project that is focused on development of an extracorporeal blood-cleansing microdevice that rapidly clears blood of pathogens. This device uses microscopic ‘magnetic opsonins’ and a combined micromagnetic-microfluidic clearance technology, which functions like an ‘artificial spleen’ to capture and remove these bound microbes, restore homeostasis, and thereby make blood-borne infections responsive to conventional antibiotic therapy.
This ongoing research and development programme, which has been funded by the Center for Integration in Medicine and Innovative Technology (CIMIT), also involves Chong Yung at the Children’s Hospital and the pair’s collaborator, Jason Fiering at Draper Laboratory, as well as a team of experienced clinicians, engineers and biomedical device developers.
This new cell-separation microdevice seamlessly integrates immunomagnetics and microfluidics. Immunomagnetic bead technology utilises nano- or micro-scale magnetic beads coated with antibodies or other specific ligands to bind targets of interest and confer magnetic mobility to those bound targets. Therefore, when pathogens lurking in the dense mixture of proteins and cells within whole blood are bound to these magnetic microparticles, they can be specifically removed by application of an external magnet field gradient. Microfluidics technology provides a means to carry out this magnetic separation in flowing blood.
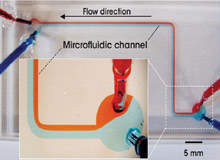
At the microscopic scale of a single microfluidic channel, fluid flows are exclusively laminar, which means that when two different streams of fluid join together, the streams flow side by side without mixing, as if there were an invisible wall dividing them, as shown in Figure 1, p93. The blood cleansing device design, as in Figure 2, leverages this unique property of laminar flow. Whole blood is removed from the vein of a patient and mixed with magnetic microbeads coated with ligands (antibodies) that specifically bind to the pathogens. It is then flowed through a microfluidic channel next to a flowing isotonic saline collecting solution.
When a magnetic field gradient is applied perpendicularly to the flow, blood pathogens bound to the magnetic beads are pulled across the laminar stream into the flowing collection fluid, which is then discarded. This process cleanses the flowing blood, which is subsequently returned to another vein of the patient in a continuous flow system. It is analogous to existing clinical extracorporeal systems used for continuous veno-venous hemofiltration (CVVH) or extracorporeal membrane oxygenation (ECMO).
Micro-cleaners: cheap and robust
Because of their small size, multiple microfluidics devices of this type created with microfabrication techniques may be oriented in parallel, and in tandem, within a single integrated laminar flow network that can clear blood of pathogens at high throughput. Moreover, since the collected pathogens continuously flow out of the device, the capacity of this pathogen filter is unlimited. This micromagnetic-microfluidic separation technology can therefore potentially be used to create robust devices that may be mass produced and made available at low cost as point-of-care devices worldwide, including in underdeveloped nations.
The proof of principle for this approach was demonstrated in 2006 when a prototype blood cleansing device composed of a single microchannel created in polydimethylsiloxane polymer was developed that used a high gradient magnetic field concentrator integrated within the system during microfabrication to perform magnetic cell separations. Using 130nm superparamagnetic beads, the device was able to achieve 80–90% clearance efficiency of E. coli bacteria from an isotonic saline solution containing red blood cells at a density similar to blood when flowing at a rate of 25–30uL/hr in a single pass.
In more recent unpublished studies, this technique has been refined to cleanse human blood of pathogenic fungi. Fungal infections were targeted because conventional anti-fungal therapies are of limited use in treating sepsis due to dose-limited systemic toxicities. Preliminary in vitro results look extremely promising as the group has been able to demonstrate efficient clearance of living fungi (C. albicans) from whole human blood and to enhance throughput a thousand-fold in their newest versions of the device.
Innovative isolation technology
The goal is to develop a device containing multiplexed microfluidic and electromagnetic devices that will cleanse the entire blood volume of a human patient of deadly pathogens within a few hours. The same technology may provide a new platform to cleanse blood of patients with leukaemia who are undergoing ‘blast crises’, in which the level of tumour cells in the circulation is so high that infarcts can occur. It also may provide an efficient way to collect circulating stem cells for regenerative medicine applications.
This research has uncovered an exciting new platform technology for isolation of living cells from biological fluids. Soon the implications of sepsis and the increasingly fatal repercussions of the disease could be a thing of the past.
