
The global healthcare system has found itself under immense strain over the past year and a half. As Covid-19 laid waste to the industry’s usual time and resources – the majority of which were redirected to caring for patients seriously ill with the then-novel respiratory virus – many patients found their elective and non-emergency surgeries had been indefinitely postponed.
In England, NHS data suggests 5.12 million people were on waiting lists to start surgical treatment at the end of April, the highest number since records began in August 2007.
Go deeper with GlobalData

Discover B2B Marketing That Performs
Combine business intelligence and editorial excellence to reach engaged professionals across 36 leading media platforms.
The detrimental effect this has had on the provision of medical and surgical training has become increasingly apparent.
A study in the International Journal of Surgery found that, across the UK and Republic of Ireland, the pandemic has had a negative impact on surgical training across all grades and specialities, with only 9% of trainees saying they would definitely meet all required competencies.
Moreover, a review in trainee logbooks shows a 50% reduction in operations with trainees as the primary operating surgeon between 2019 and 2020.
The long-term implications of these figures for workforce retention, recruitment and progression are unknown, but even a temporary reduction in the number of graduating surgeons is unlikely to spell good news for the healthcare system.
But simulated surgery is opening the doors for students to keep training and for qualified clinicians to learn about new tools and procedures, even as the pandemic continues. These platforms were already growing in popularity before 2020, but Covid-19 has acted as something of a catalyst for remote technologies across the healthcare industry, and remote surgical training is no exception.
A new £1m teaching hub is now set to launch in Wrightington, West Lancashire, to allow surgeons to train remotely using immersive technology. Known as the Technology Enhanced Learning (TEL) Centre, the facility will deliver enhanced remote training for both trainee doctors and senior clinicians to practice medical procedures.
This will be done using a combination of virtual reality (VR), augmented reality (AR) and mixed reality (MR). The sessions will also be beamed to several centres across the UK simultaneously.
With funding pouring into the remote surgical training sector, Medical Technology asks what this could mean for medical students?
Tactile training
There are several different approaches out there when it comes to digital surgical training, from Level Ex’s gamified solutions to training simulators with a more tactile element.
VirtaMed uses anatomical rubber models of different body parts on which surgeons can practice arthroscopic operations, with photorealistic AR graphics displayed on-screen.
VirtaMed vice-president of marketing Phil Norris says: “Inside the anatomical model of the knee, for example, we’ve got the bone structure, so when the surgeon is operating, they feel the pressure of the instrument against the bone.
But the most compelling thing is the visual graphics. This allows us to simulate basically any pathology, and we can do these with the same anatomical model, showing different complications, different ways that a surgeon could do the procedure, and giving some AR guidance as well.”
During the height of the pandemic, restrictions meant that many hospitals would not allow medical educators onto the premises. As a result, Norris rented a moving van and set up a mobile teaching unit, visiting the car parks of Switzerland’s teaching hospitals to provide training.
“Because we’re dealing mainly with hands-on training here, the pandemic looked to be catastrophic to us because we were being encouraged not to meet together,” he says.
“The compromise was that we rented a truck and put the simulators inside, and the residents were allowed out for certain periods during the day to do training with us. Many of them weren’t getting that time in the operating room, even just as observation time, so this was a great way of them getting some hands-on training that they wouldn’t have had otherwise.”
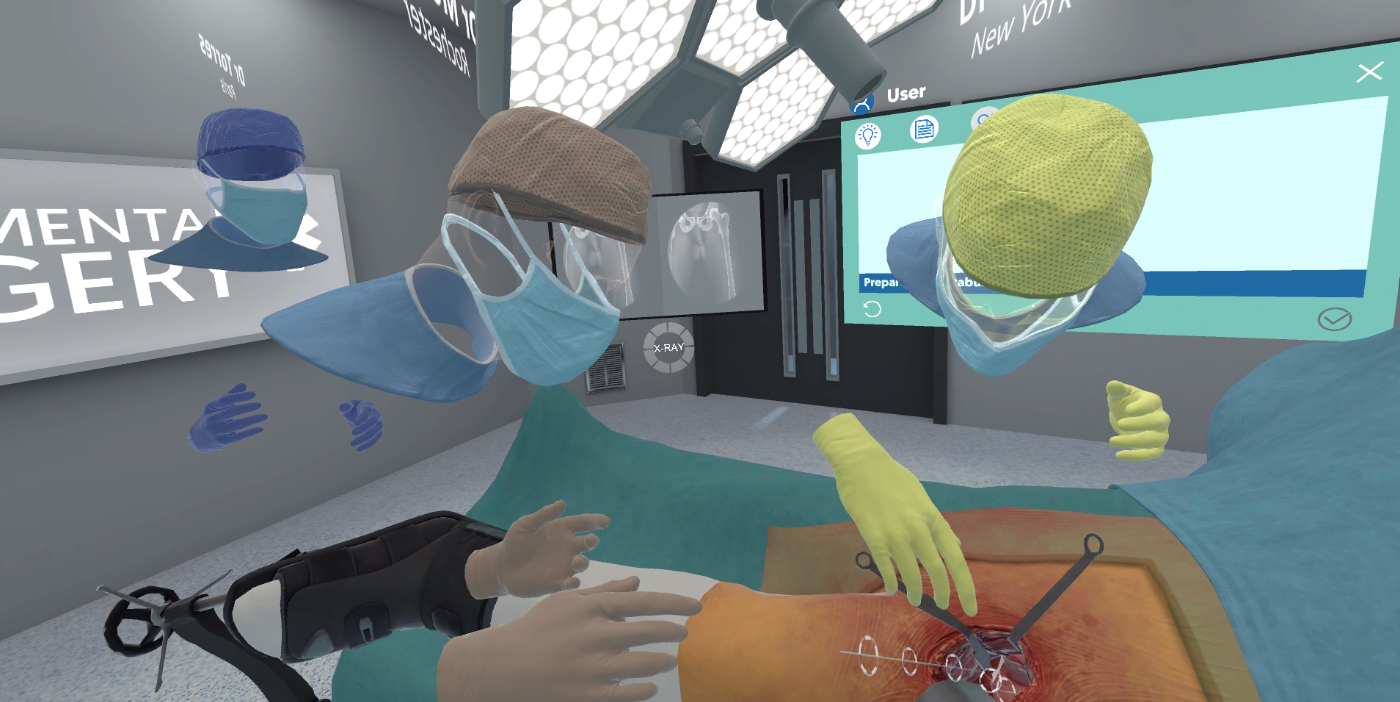
FundamentalVR takes a slightly different approach to VirtaMed, but centres haptic feedback within its design. With the aim of becoming a ‘flight simulator for surgery’, the company’s Fundamental Surgery VR platform provides surgical trainees with simulations of the same physical cues they would experience during a real procedure.
Fundamental Surgery doesn’t utilise anatomical models like VirtaMed. Instead, it simulates the inside of an operating room through a VR headset while handheld instruments deliver kinaesthetic feedback. As users interact with the virtual patient, they get the same physical feedback they would in a real-life environment.
FundamentalVR CEO and co-founder Richard Vincent says: “It can be configured in lots of different ways, depending on where you are in your medical journey. We don’t tend to focus too much on early-stage training, where we really come alive is further along in your developmental cycle.
“Within any medical realm, continuous professional development is essential. I could be a 20+ year qualified surgeon, I’ve still got to understand and keep up to date with different processes.”
Democratisation or wealth gap creation
Virtual surgical training could potentially help to democratise access to surgical training in rural or resource-limited settings. In these areas, patient volumes in a hospital may not be as high as in more urban or wealthy territories, meaning surgical trainees will have limited access to the number of cases they need to experience before qualifying.
Vincent says: “With our system, you can use a headset that costs less than £500, send it by post and [surgeons and trainees] can collaborate straight away. It’s a great way of democratising, lowering the costs and providing access.
“Orbis, the eye charity, is one of our partners and clients. Their whole mission is about teaching cataracts procedures. The biggest challenge is how do you train people in those outback areas in what is really quite a simple procedure? Now you can send our system out and it can train them without anyone having to travel there.”
Remote surgical training could thus allow students who usually wouldn’t have access to certain training programmes to broaden their skillset. However, it’s important not to think of virtual training as a silver bullet to solving this problem.
There’s a risk that virtual training could actually lead to a treatment wealth gap within resource-limited areas, where only certain students are able to access these novel technologies and in turn only more affluent members of the population can afford their services.
“The relative costs are small, but obviously when you say, ‘it’s just a £500 headset’ and you take that to a third world country, that’s a lot of money,” Vincent says. “I think there’s a little bit of funding that needs to flow from charities and the World Health Organisation to try and facilitate the pushing out of surgical skills.”
The benefits of virtual training
Virtual surgical training has a number of other benefits outside of allowing professional development to continue during the pandemic, like improving upon several elements of cadaver training.
“Cadaver training is historically one of the gold standards in surgical training, but they have some limitations,” says Norris. “They don’t bleed in the same way an alive patient does, which we can simulate. You can only really use a cadaver once, twice, maybe three times, whereas simulation provides unlimited training.
“Also, I think the mentality is different with a cadaver. You still want to respect that body that’s in front of you, whereas with a simulator you don’t mind experimenting, and I think experimentation is where a lot of learning comes from.”
Virtual training also provides a way to expedite the learning process. A study published last August in Clinical Orthopaedics and Related Research found that VR increased procedural accuracy and completion of an intramedullary tibial nail procedure, compared to traditional training techniques.
Another study, conducted at the University of California Los Angeles and presented at the 2019 Current Annual Meeting of the Western Orthopedic Association, showed a 230% improvement in participants’ overall surgical performance when prepared with VR training.
It’s clear that VR, AR and MR have a role to play in the future of surgical training – pandemic or no pandemic. While no surgical resident is going to bounce straight from a few sessions on a simulator to heading up an operating room, simulators may help them build skills more quickly and efficiently.
Vincent says: “The old adage is that practice makes perfect. If you can rehearse a surgical procedure 100 times in a day, as opposed to twice, you can practice and refine your skills. It’s more cost effective, and the human cost of making a mistake inside a live patient is enormous. Two years ago, the UK compensation for medical errors was £1.6bn. Anything that removes that improves patient outcomes.”
